

20 Oct Deep Brain Stimulation for Parkinson’s: A Guide to the Procedure, Benefits, and Common Misconceptions
Deep Brain Stimulation for Parkinson’s: A Guide to the Procedure, Benefits, and Common Misconceptions
By Island Hospital | October 20, 2025 10:34:09 AM
Living with Parkinson’s disease can be overwhelming, not only for patients but also for their families. Imagine being unable to hold a cup of tea without spilling, freezing mid-step while trying to cross a room, or struggling to write your own name with steady hands.
For many people living with Parkinson’s disease, these challenges are part of everyday life. To make matters more complicated, medications that once worked well may gradually lose their effectiveness over time. This often leaves patients and families searching for new solutions.
One of the most promising options is Deep Brain Stimulation (DBS), a well-established, FDA-approved surgical procedure that has been used safely for decades. DBS helps manage the symptoms of Parkinson’s disease, providing many patients with renewed independence and confidence in their daily lives.
Yet despite its proven track record, DBS is often surrounded by myths and misconceptions. Some believe it’s a cure, while others fear it is unsafe or untested. In this article, we’ll uncover the myths, truths, and facts about DBS, so you can make an informed decision if you or your loved one is considering this treatment.
What is Deep Brain Stimulation (DBS)?
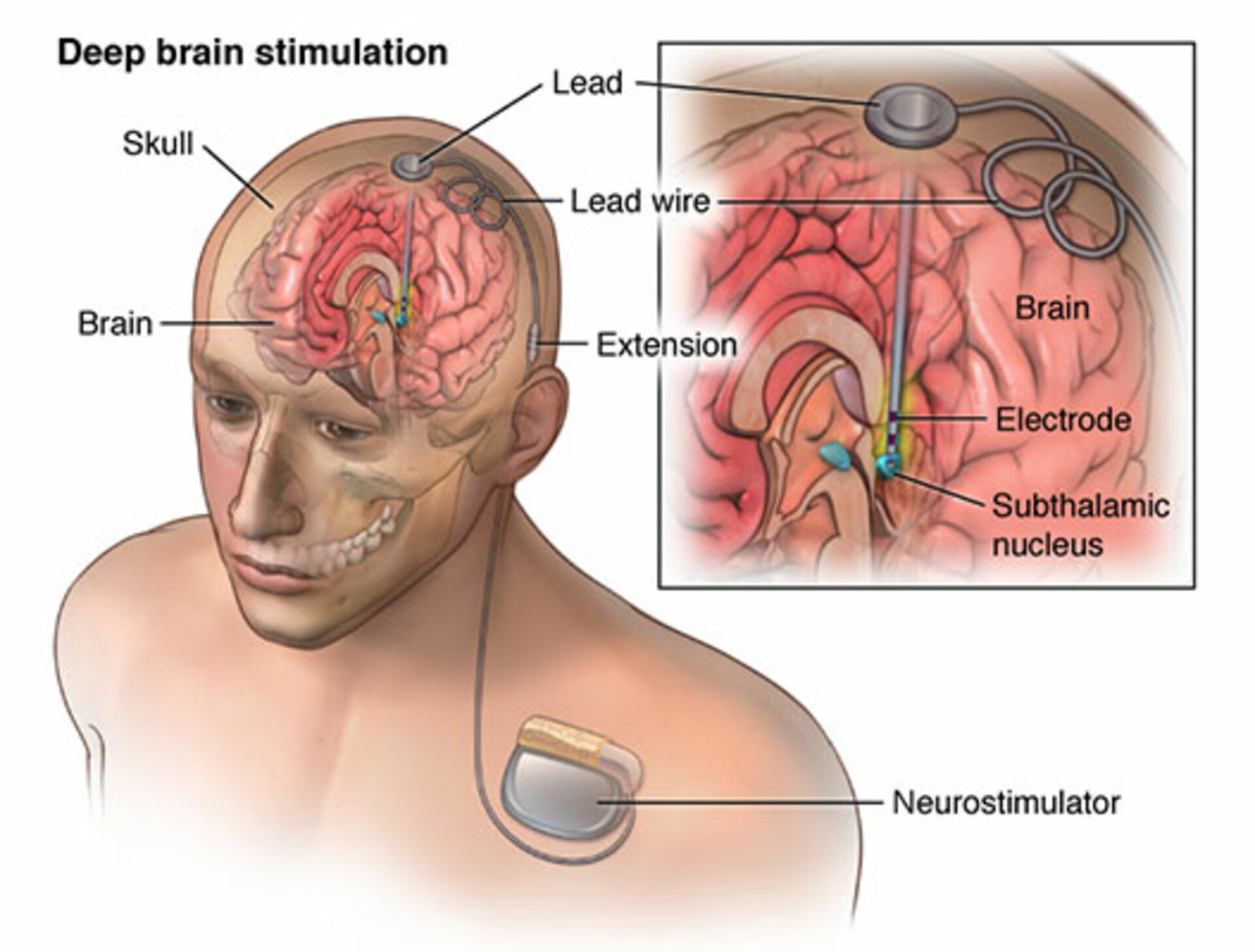
Deep Brain Stimulation (DBS) is a well-established surgical treatment that helps manage the symptoms of Parkinson’s disease and other movement disorders. The procedure involves implanting a small, pacemaker-like device under the skin of the chest
This device delivers mild electrical impulses through thin wires (called electrodes) that are placed in specific areas of the brain responsible for movement control. These impulses help regulate abnormal brain activity, easing symptoms such as tremors, stiffness, slowness, and difficulties with movement.
DBS has been used safely for decades around the world and is recognised as a standard treatment by major health authorities.
While most commonly used for Parkinson’s disease, DBS is also effective in treating essential tremor, dystonia, epilepsy, and obsessive-compulsive disorder (OCD). Importantly, DBS is not a cure for Parkinson’s, but its goal is to improve quality of life by reducing disabling symptoms and restoring independence in daily activities.
Myths, Truths and Facts about Deep Brain Stimulation by Dr Lim Thien Thien & Dr Lee Hock Keong
The Truth About Deep Brain Stimulation: Debunking the Myths and Facts
Although Deep Brain Stimulation (DBS) has been safely performed for decades and is recognised as a standard treatment for Parkinson’s disease, many patients and families remain hesitant because of lingering misconceptions.
Some believe it is a cure, while others worry the surgery is dangerous or still experimental. These misunderstandings often create unnecessary anxiety and may even prevent patients from considering a treatment that could greatly improve their quality of life. Let’s put the rumours to rest and start debunking!
Myth 1: DBS is a cure for Parkinson’s disease
Fact: Unlike what some may believe when the topic of DBS comes up, DBS does not cure Parkinson’s disease, nor does it stop the condition from progressing.
What it does is help manage symptoms that medication alone can no longer fully control, particularly tremors, stiffness, slowness, motor fluctuations, and movement difficulties. This allows many patients to live more independently and comfortably.
Why this matters: Many patients experience dramatic improvements in daily life after DBS, such as steadier hands, smoother walking, and fewer “off” periods, even though the disease itself continues to progress.
Myth 2: DBS is only for late-stage, bedridden patients
Fact: Because DBS is not recommended as the first line of treatment like medication, many people assume it is only offered in the most critical stages of Parkinson’s disease. However, this is not true.
DBS is not reserved for late-stage patients. In fact, those who are already bedridden or extremely frail are usually not suitable candidates. Instead, DBS is considered when medication no longer controls symptoms well, or when “on-off” fluctuations and involuntary movements (dyskinesias) become disruptive.
The procedure is most effective for patients in the mid-stages of Parkinson’s, usually after about five years of diagnosis.
Why this matters: Viewing DBS as a “last resort” can cause patients to miss the window when they could benefit most. With proper timing, DBS can restore independence, reduce the need for high medication doses, and improve quality of life for many years.
Myth 3: The surgery is dangerous and involves a large opening in the skull
Fact: Many people picture brain surgery as something highly invasive and risky, but DBS is actually considered a low-risk procedure when performed by experienced neurosurgeons. Instead of a large opening, the surgery requires only a small hole in the skull to insert thin electrodes into very specific areas of the brain.
The neurostimulator (similar to a pacemaker) is then placed under the skin of the chest, connected by wires tunnelled discreetly under the skin.
Why this matters: Understanding that DBS is a minimally invasive and highly precise surgery can help reduce fear. While, like any surgery, there are risks such as infection or bleeding, these are rare. In most cases, DBS is safe and well-tolerated, with patients typically discharged from the hospital within just a few days.
Myth 4: You won’t need medication after DBS
Fact: Because DBS is sometimes mistaken as a cure or a last-resort treatment, many people also assume that medication is no longer necessary after the procedure. This is not true.
While DBS is highly effective in reducing motor symptoms, it does not replace Parkinson’s medication entirely. Most patients still take medication, but often at a much lower dose, sometimes reduced by 50–70%. This not only keeps symptoms under control but also minimises side effects caused by long-term or high-dose medication use.
Why this matters: Believing that DBS completely eliminates the need for medication can set unrealistic expectations. The real benefit of DBS is that it works in partnership with medication, helping patients achieve smoother, more consistent symptom control and a better quality of life.
Myth 5: You have to be awake during surgery
Fact: In the past, DBS surgery often required patients to be awake so surgeons could test the placement of electrodes and the effects of stimulation in real time. Understandably, this idea can feel intimidating.
However, thanks to modern imaging and surgical techniques, DBS can now be performed safely under general anaesthesia. This means patients are completely asleep during the procedure, making the experience far less stressful.
Why this matters: Knowing that you don’t have to be awake for surgery can ease much of the fear and anxiety surrounding DBS. For many patients, this reassurance makes the treatment feel more approachable and less daunting.
Myth 6: DBS is experimental
Fact: DBS is far from experimental. It has been in use for over three decades and is an FDA-approved treatment for Parkinson’s disease and other movement disorders. More than 160,000 patients worldwide have undergone DBS, and countless studies confirm its safety and effectiveness.
Today, DBS is widely recognised as a standard of care for conditions like Parkinson’s, essential tremor, and dystonia.
Why this matters: Thinking of DBS as “experimental” may discourage patients from considering a proven treatment that could significantly improve their quality of life. Understanding that DBS is a trusted, established therapy helps patients and families feel more confident when exploring their options.
Myth 7: DBS is only for Parkinson’s disease
Fact: While DBS is most commonly used to manage symptoms of Parkinson’s disease, it is not limited to only this condition. DBS has also been proven effective in treating essential tremor, dystonia, epilepsy, and obsessive-compulsive disorder (OCD).
Its proven success across different conditions reinforces its reputation as a safe and versatile treatment.
Why this matters: Believing that DBS is “only for Parkinson’s” can cause patients with other conditions to overlook a treatment that could help them. Recognising its broader applications allows more people to explore DBS as a potential solution to improve their daily lives.
Myth 8: DBS will change my personality or make me emotionless
Fact: DBS is designed to regulate abnormal brain signals that cause movement problems, not to alter who you are. While some patients may experience mild mood changes, DBS does not erase emotions or change personality.
The device is carefully programmed and adjusted after surgery to suit each patient’s needs, ensuring both safety and comfort. In the hands of skilled neurosurgeons, DBS is a safe and precise therapy.
Why this matters: Fearing that DBS will affect personality or emotions may cause unnecessary worry.
Myth 9: Everyone with Parkinson’s disease is a candidate for DBS
Fact: Not all patients with Parkinson’s disease are suitable for DBS. The best candidates are typically those who have had the condition for at least five years, experience disabling tremors, severe motor fluctuations, or dyskinesias, and whose symptoms are no longer well controlled by medication.
Patients with significant cognitive decline, advanced frailty, or other serious health conditions may not be good candidates either.
Why this matters: Believing that DBS works for everyone can lead to false hope or disappointment. The reality is that careful evaluation by a neurologist and neurosurgeon is essential to determine whether DBS is the right option.
Myth 10: DBS makes you dependent on the device
Fact: DBS is recommended to help manage movement symptoms, but that doesn’t mean you are “stuck” with it forever. DBS does not create dependence in the way many people fear. The device is designed to support your brain’s natural function by regulating abnormal signals that cause movement problems.
It can be turned off, reprogrammed, or even removed if necessary. Patients can still function without the device, though their symptoms will return. Far from making patients dependent, DBS often reduces the need for medication and helps people regain independence in daily life.
Why this matters: The idea of being “tied” to a device can sound intimidating, but the reality is very different. DBS is adjustable, reversible, and always tailored to the individual’s needs, empowering patients rather than limiting them.
Living with Parkinson’s can be challenging, but you don’t have to face it alone. Ask our Parkinson’s specialists your questions and explore treatment options today.
The DBS Patient Journey: From Consultation to Recovery

By now, we have cleared up many of the common doubts and misconceptions about DBS, and you may be wondering what the actual journey looks like. So, let’s switch gears. What really happens if you decide to undergo DBS? From consultation to recovery (and everything in between), here’s a closer look at what you can expect along the way.
1. Patient suitability: Who is a good candidate for DBS?
DBS isn’t right for everyone with Parkinson’s disease. Doctors carefully assess each patient to ensure the treatment will be both safe and beneficial. In general, good candidates are those who:
- Have been diagnosed with Parkinson’s disease for at least five years
- Struggle with disabling tremors, dyskinesias, or severe motor fluctuations
- Experience “on-off” periods that can’t be controlled, even with careful adjustments to medication
- Live with significant dyskinesias (involuntary movements) and frequent “wearing off” or “off-time” episodes throughout the day
Careful patient selection ensures that DBS is used at the right time, for the right people. Patients who meet these criteria are far more likely to see meaningful improvements in movement, independence, and quality of life.
2. The surgical procedure: What to expect
Undergoing DBS can feel like stepping into the unknown, but knowing exactly what happens can bring peace of mind. Here’s a step-by-step overview of how the surgery works when it’s done under general anaesthesia:
Before Surgery
- Pre-operative assessments
You’ll meet with a team including a neurologist, neurosurgeon, psychiatrist, and neuropsychologist. They’ll check whether DBS is a good fit for you.
- Brain imaging
You’ll have MRI scans, one with contrast (gadolinium) and one without, to map your brain accurately. These images help the surgical team pinpoint exactly where to place electrodes. Sometimes, mild sedation is used if needed.
- Surgical planning and committee review
A multidisciplinary team reviews your case to ensure you’ll benefit from DBS. If approved, they’ll schedule the surgery and walk you through what to expect.
- Preoperative instructions
Before the day of surgery, you’ll meet with anaesthesiology and neurosurgery teams, sign consent forms, get instructions on fasting, and be told which medications you may need to stop.
During Surgery
- Electrode placement
A small portion of the head may be shaved, and local numbing applied before surgery begins. Once under general anaesthesia, the neurosurgical team makes tiny openings in the skull, called “burr holes.”Through these openings, thin electrodes are gently placed into precise areas of the brain, guided by advanced MRI imaging for accuracy.
- Device implantation
About a week later, once the brain electrodes are in place, a second procedure is performed. During this stage, the neurostimulator (battery pack) is placed under the skin near the collarbone and connected to the electrodes with thin wires. This surgery is also done while you are asleep under general anaesthesia, usually lasting around 2½ hours. Most patients can go home the very next day.
After Surgery
- Initial programming
Roughly two weeks after the device is implanted, you’ll return for the first programming session. Medications may be paused briefly so the team can fine-tune stimulation settings to get symptom relief. This session can last up to a few hours.
- Fine-tuning period
Over the next 3-6 months, you’ll have several follow-ups to adjust stimulation levels and check battery status. These visits are more frequent during this period. As you stabilise, visits become less frequent.
- What to expect in recovery
It’s common to feel a bit disoriented or confused in the first few days after surgery; this is temporary. Some improvements (like tremor control) may appear immediately, but others take time, maybe weeks to months, as your brain adjusts.
3. Life After DBS: Recovery and Adjustment
DBS surgery is only the beginning of the journey. What comes next is a period of healing, rest, and gradual adjustment as your body adapts to the changes.
Recovery doesn’t happen overnight; it’s a step-by-step process that looks a little different for everyone. With proper care and support, most patients steadily move toward greater independence and a better quality of life.
- Rest and Healing
In the first few weeks, your body needs plenty of rest. Some swelling, soreness, or bruising around the incision sites is normal and usually improves with time. It’s important not to overexert yourself. Light activity is encouraged, but heavy lifting or strenuous exercise should be avoided until your doctor clears you. - Managing Fall Risk
Balance may be a little unsteady in the early recovery period, especially as your care team adjusts medications and stimulation settings. To stay safe, patients are often advised to use mobility aids (like a cane or walker) and take extra care on stairs and uneven ground. Fall prevention at this stage is key to long-term recovery. - Symptom Adjustment
Some patients notice immediate improvements after surgery, while others experience temporary ups and downs before the full benefits of DBS are realised. This is normal. It can take weeks to months for your care team to fine-tune your treatment, so patience is essential. Gradually, tremors, stiffness, and “off” periods usually become much easier to manage. - Recovery Time
Everyone recovers at their own pace, but most patients start feeling more stable and confident within a few months. By this time, many notice a significant difference in daily activities, whether it’s walking more smoothly, enjoying meals without tremor, or having more “good” hours in the day.
Taking a proactive approach to your health starts with effective screening. Discover how to best prepare for your health screening in this comprehensive guide.
Explore Whether DBS Is Right for You!
Deep Brain Stimulation (DBS) is not a cure for Parkinson’s disease, but it is a proven, safe, and effective treatment that can greatly improve quality of life for the right patients. Understanding the difference between myths and facts is key to building clarity and confidence when considering DBS.
At Island Hospital, our Neurology and Neurosurgery team works closely with each patient and family to ensure the right treatment plan is chosen, with safety, compassion, and expertise at every step. If you or a loved one is considering DBS or wants to explore whether it may be the right option, we’re here to help.
Ready to start your journey with us? Book a consultation with us today!
FAQs
1. Does DBS require frequent battery replacement?
No. Most DBS systems are designed to last for several years before the battery needs replacement. Standard non-rechargeable batteries usually last 3–5 years, depending on how much stimulation is required.
Rechargeable systems can last 10–15 years with regular charging. When a replacement is needed, the procedure is minor compared to the original surgery and typically involves only replacing the battery pack, not the brain electrodes.
2. How much does DBS cost in Malaysia?
The cost for DBS in Malaysia can vary widely depending on the hospital (private vs government), the type of device used, and the complexity of each patient’s situation.
Roughly, the prices range:
- In private hospitals in Kuala Lumpur, costs generally range from RM 127,000 to RM 190,000
- In public or government hospitals, the cost might be lower, around RM 85,000 for the surgery alone, but additional costs for devices, follow-ups, and services will apply.
Always consult your neurosurgery team for a detailed cost estimate that includes all pre- and post-surgery expenses specific to your case.
3. Do I need to shave my head for DBS surgery?
Not completely. Only a small area of the scalp is shaved where the electrodes are placed. The rest of the hair is usually left intact, and it grows back over time.
4. What is the success rate of DBS for Parkinson’s?
DBS has a high success rate for carefully selected patients, particularly in reducing tremors, dyskinesias, and “off” periods. While results vary, many patients report dramatic improvements in independence and daily activities.
In fact, one of our patients, Mr Wang, 59, shared that DBS gave him back his ability to write and move with confidence. Watch his testimonial here!
5. How long after DBS can you drive?
This depends on your recovery and your doctor’s advice. Most patients need to wait at least a few weeks before resuming driving, and only after their symptoms are stable and stimulation settings are optimised. Safety always comes first, so clearance from your neurologist is essential.
Related Doctors
Latest Blog Posts

July 30, 2026

July 20, 2026

July 18, 2026